
Burt/Paquette Oral Boards
Case 1. Patient had carbon monoxide poisoning with an ischemic appearing EKG. Patient has criteria for hyperbaric treatment.

* Criteria for Hyperbaric Therapy for CO poisoning (#4 from bottom)
Case 2. 68yo male developed V-fib in the setting of hypokalemia and pneumonia.

*V fib
Patient was defibrillated to sinus rhythm but remained unresponsive. Consequently patient needed to receive therapeutic hypothermia.
Elise made the point that the appropriate order of response to V-fib is Ciculation, Airway, Breathing. Circulation first with CPR and defibrillation. After you address circulation then move to airway with an LMA if needed and then breathing.
Case 3. 24 year old female with foot pain. Patient twisted her foot while dancing.
Xray shows pseudo-jones fracture
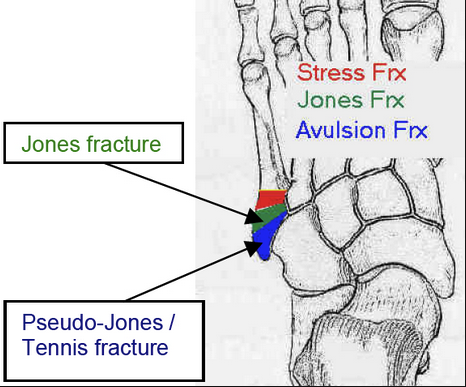
*Jones vs Pseudo Jones fracture

*Jones vs Pseudo Jones fracture
Shannon Staley MD ACMC Pediatric EM Faculty Why Kids are not Small Adults
Case 1. 22mo with head injury. No loss of consciousness but more fussy since injury. Child has a frontal hematoma. Should you scan or not? It is estimated that around 5000 cases of cancer may result from the 4 milliion CT scans done on kids per year. The Choosing Wisely Campaign promotes doing less head CT’s in children for head injury. Shannon advised using the PCARN guidelines to help make decisions on head-injured children.

*PCARNHead Injury Rule

*PCARN Head Injury Rule A reasonable observation period is 6 hours from time of injury.

*TEN-4 Bruising Rule. If you identify any of these types of bruises in an injured child, you need to investigate the injury a bit further to figure out if there was non-accidental trauma.
Case 2. 10 month old male with cough, congestion, wheezing in the winter time. Diagnosis is bronchiolitis. The go-to treatment for bronchiolitis is suctioning. If there is overt wheezing , you can try 4 puffs with an albuterol mdi with a spacer and mask. If the child improves, home use is worth a try.
In hypoxic patients, hi flow O2 is a good option.
Which kids end up in the PICU? Children under age 2 with history of low birth weight kids (<5 lbs) and current RR>70. Low birth weight kids are more prone to delayed lung development. For full term kids admit all under 3 months of age for risk of apnea.
Don’t get CXR on kids with bronchiolitis unless you suspect pneumonia for some reason.
Give supplemental O2 for Pulse Ox <90%
No need to send PCR testing for RSV. Testing does not change management.
Case 3. 7.5-week infant with fever to 101.2. Child looks ok. WBC is 11. UA shows signs of UTI. 6.5% of UTI’s at this age will have bacteremia. 2.8% of febrile neonates with uti will have serious neurologic complications such as meningitis or require intubation. We had an animated debate about how much of a work up these kids need to have. Many faculty wanted to do a limited septic work up in such a child with no LP. However, everyone agreed that 2.8% rate of serious neurologic complications is concerning and makes you think twice that maybe doing an LP is more indicated than we thought.
Case 4. Shannon discussed complications of septic joints. The main point was that septic joint patients can get severely septic and possible die or loose a limb more rapidly than you would expect. If you suspect septic joint and there will be a delay to joint aspiration for several hours, she recommends giving IV antibiotics to cover MRSA and MSSA.
Regan/Kennedy/Holland/Cartalano/Omi Thoracic Trauma
200,000 Americans die every year from trauma. 50,000 of those are from thoracic trauma. 1/3 of deaths due to thoracic trauma occur prior to arrival to hospital. Another 1/3 of these deaths occur in the first 1-3 hours after arrival to hospital. The main causes of early death are aortic injury, cardiac injury/pericardial tamponade, and airway obstruction/aspiration.
Fractures of ribs 1-3 suggest hi energy injury. Lower rib fractures suggest lung and diaphragm injuries. Diaphragm can move as high as the 4th intercostal space on expiration.

*Cardiac Box
The most common area of aortic injury is at the take off from heart. This location of injury is always fatal. The most common area of survivable aortic injury is just distal to the left subclavian artery because the aorta is tethered there.
Unfortunately, I was called out for a large portion of this excellent lecture, so the notes are missing a lot of info.
Harwood Reference: Blunt Cardiac Injury, Screening for
Published 2012
Citation: J Trauma. 73(5):S301-S306, November 2012
Level 1
An admission electrocardiogram (ECG) should be performed on all
patients in whom BCI is suspected (no change).
Level 2
If the admission ECG reveals a new abnormality (arrhythmia, ST changes,
ischemia, heart block, and unexplained ST changes), the patient should
be admitted for continuous ECG monitoring. For patients with
preexisting abnormalities, comparison should be made to a previous ECG
to determine need for monitoring (updated).
In patients with a normal ECG result and normal troponin I level, BCI
is ruled out. The optimal timing of these measurements, however, has
yet to be determined. Conversely, patients with normal ECG results but
elevated troponin I level should be admitted to a monitored setting
(new).
For patients with hemodynamic instability or persistent new arrhythmia,
an echocardiogram should be obtained. If an optimal transthoracic
echocardiogram cannot be performed, the patient should have a
transesophageal echocardiogram (updated).
The presence of a sternal fracture alone does not predict the presence
of BCI and thus should not prompt monitoring in the setting of normal
ECG result and troponin I level (moved from Level 3).
Creatinine phosphokinase with isoenzyme analysis should not be
performed because it is not useful in predicting which patients have or
will have complications related to BCI (modified and moved from Level
3).
Nuclear medicine studies add little when compared with echocardiography
and should not be routinely performed (no change).
Level 3
Elderly patients with known cardiac disease, unstable patients, and
those with an abnormal admission ECG result can safely undergo surgery
provided that they are appropriately monitored. Consideration should be
given to placement of a pulmonary artery catheter in such cases (no
change).
Troponin I should be measured routinely for patients with suspected
BCI; if elevated, patients should be admitted to a monitored setting
and troponin I should be followed up serially, although the optimal
timing is unknown (new).
Cardiac computed tomography (CT) or magnetic resonance imaging (MRI)
can be used to help differentiate acute myocardial infarction (AMI)
from BCI in trauma patients with abnormal ECG result, cardiac enzymes,
and/or abnormal echo to determine need for cardiac catheterization
and/or anticoagulation (new).
Pulmonary contusions are treated based on age and severity of contusion. Dr. Cartalano advised ICU observation, aggressive pain control, judicious IV fluids, bipap and intubation if needed. The pulmonary contusion will be at it’s worst on day 3. If the patient is in distress on day 1 they likely will need intubation to survive day 3.
Flail chest requires 3 or more consecutive ribs with segmental fractures. It is problematic mostly for the underlying pulmonary contusion. Treat the pulmonary contusion as noted above. There is debate among Traumatologists about the utility of internal fixation of the fractured ribs causing flail chest.
If intubating for thoracic trauma use a lung protective strategy of low tidal volume of 6-8 ml/kg, and PEEP titrated to maintain oxygenation.

*Lung Protective Strategy

*Needle decompression of tension pneumothorax. Trauma surgeons also said that if you can’t find a 3-inch catheter, just put in a chest tube if you suspect a tension pneumothorax.
Definition of massive hemothorax is 1500ml of blood into the chest tube initially or 200ml of blood output per hour for 4 hours. Patients meeting this criteria should go to the OR.
We had a robust discussion on ED Thoracotomy. Trauma faculty felt that if you are an emergency physician in an ED with no thoracic surgery back up, don’t ever do a thoracotomy. Even if you can fix the problem with thoracotomy, you need some one to definitively treat the surgical problem. If these patients get transferred with open chests they won’t survive. If you have Trauma or Thoracic surgery back-up where you are working then consider following an algorithm such as the one below.

*Decision to Perform ED Thoracotomy
Tekwani/Watts Research in Residency
Reasons to do research: Confidence builder, opportunities to travel and present your work, networking, career builder.
5 keys to a successful resident project: Start early, brainstorm multiple clinical questions that are interesting to you, evaluate your ideas using FINER criteria (see below), find a friend to collaborate on projects with, create and follow a timeline. Pick an appropriate journal for publication.
Feasible
Interesting to you and the EM community
Novel: Based on literature search
Ethical
Relevant: Does it pass the “so what ?“ test
“Easy” IRB studies are “hands off” studies: chart reviews, education research, meta- analysis, etc.
“Difficult” IRB studies involve potential harm or cost to patients, RCT’s, studies on critically ill patients.
IRB approval not required: QI studies, Case reports, Image submission.