
Barounis Hypoxemic Respiratory Failure
Peak pressure is calculated on resistance and flow.
Plateau pressure is calculated on tidal volume and compliance. There is no flow in the measurement of plateau pressure. You get a plateau pressure when the ventilations are paused.
If peak and plateau pressures are both high then you have a compliance problem.
Compliance is affected by water, pus, air, or blood in the lung, or fat compressing the lung.
If the peak pressure is high and the plateau pressure is normal then there is a resistance/flow problem. Think mucous plug or kinked ET tube or bronchospasm or right mainstem intubation.
Lungs are very sensitive to high plateau pressures. As noted above, plateau pressure is affected by tidal volume. High Tidal volumes have been found to cause ARDS.
Obesity can affect lung compliance. It is important to put the patient in reverse trandelenburg (feet down, head up) to displace the stomach off the diaphragm.
Dave made the point: Use Low Tidal Volumes in All Patients
For most male patients a TV of 500 is a reasonable starting point. In most women a TV of 400 is a reasonable starting point. You have to give a slightly higher respiratory rate around 16 when using these lower tidal volumes. Start with 5 of PEEP but you can go up to 10 or 12 if patient is still hypoxic. Of course, asthmatic patients will need lower ventilation rates.
Don’t give a lot of fluids to patients with ARDS. They will third space fluid into their lungs. Dave wants to keep his ARDS patients as dry as possible. In fact intensivists are using a lot of Lasix in ARDS patients to keep them as dry as possible.
Inhaled nitrous oxide can be useful to improve VQ mismatching. Nitrous oxide improves the measurements of lung function but it has not been shown to improve mortality.
For refractory hypoxemia, prone positioning works to improve survival.
Finally ECMO can be life saving in a select group of severe ARDS patients.
Hart /Chan Oral Boards
Case 1. 59 yo female with abdominal pain. Vitals normal except BP of 102/52. Labs are normal except an elevated lactate. Repeat exam shows persistent pain and diffuse abdominal tenderness. Upright Chext X-ray shows free air.

*Free air on Chest X-ray
Upright Chest X-ray is 80% sensitive for free air. Give IV antibiotics, pain medication, fluids, and get patient to the OR.
Elise comment: Check an EKG on elder patients with abdominal pain. AMI can present with abdominal pain.
Harwood comment: Upper GI perforations will present early with severe pain. Lower GI perforations from a perforated diverticulum will present in a delayed fashion with less severe pain and significant amount of free air. The CT findings will seem inconsistent with the patient’s clinical presentation.
Case 2. 21 mo male refusing to walk. Vitals and Dexi are normal. Xrays show a Toddler’s Fracture

*Toddler’s fracture. These are not associated with child abuse.
Case 3. 69 yo male with an episode of near syncope. Vitals are normal. Dexi is normal. EKG shows markedly peaked T-waves.

*Hyperkalemic EKG note the Tall Narrow T waves. P waves are still present and QRS is still narrow.

*Hyperkalemic EKG changes
Patient had potassium of 6.7. He had signs of renal failure.
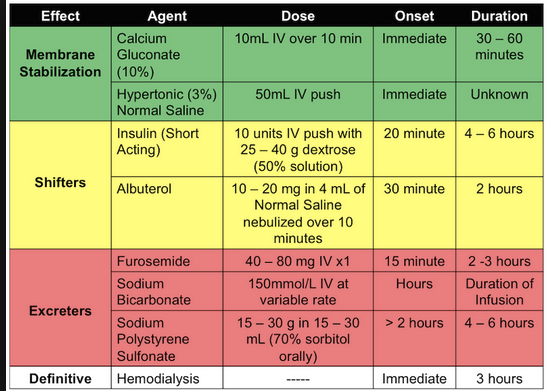
*Treatment of Hyperkalemia
Elise comment: In a male with new renal failure, use ultrasound or place a foley to identify acute urinary retention.
Katiyar Billing and Coding
Doctors are now almost universally evaluated by the RVU system. If your group generates more RVU’s, you have more money to hire physicians and make capital investments such as purchasing an ultrasound machine. If you are a low RVU generator you will be at risk to be fired.
There are two ways RVU’s are factored into physician compensation. 1. Pure RVU reimbursement. 2. As a factor in a bonus system above the guaranteed base salary.

*RVU’s per EM Code
Remember “Fortuntenate” 4-2-10-8. 4HPI factors, 2History Items, 10 ROS items, 8 physical exam items are required for a level 5 EM code.
Use the EM caveat for patients who cannot communicate effectively with you. For kids under age 6 most faculty felt it is reasonable to use the caveat for age. Our coder felt that age was problematic sometimes as an EM caveat. She said to get as much history from the parent as possible. Language barrier is not a factor that can be used to invoke the EM Caveat. You have a responsibility to get an appropriate translator. Our coder suggested that using clinical acuity as the EM Caveat is probably the best factor you can use.
Risk management issues:
1. Document “no FB” in all lacerations. Harwood comment: I document that I asked the patient if they feel any foreign body or if they are concerned there is a foreign body. I document that I looked for a foreign body. I document that the patient declined an x-ray.
2. Document “tendon intact” for all lacerations
3. Document pregnancy status in all female abdominal pain patients
4. Document re-evaluations and status of patients
5. Document time and content of conversations with PMD and Consultants
If you want the PICU attending to see a patient in the PED, put in a consult order for the PICU attending.
If you are sending images to another physician regarding patient care, be sure you have patient and family consent. Also use Perfect Serve to send the image. It is HIPPA compliant and time stamped.
Look at your all your xrays. The radiologist can miss stuff because they don’t know the clinical picture.
Nejak ED Crowding
ED Crowding is when the number of patients in the ED put such a strain on resources that ED care for patients is hampered or limited.
One thing we can do to improve patient throughput is to order antibiotics as soon as we know we are going to give them.
Elective surgeries at the beginning of the week have been identified as an important factor in ED crowding. Some are advocating 24/7 work culture for all areas of the hospital not just the ER and ICU’s. The OR’s could go 24/7 to smooth out the weeks’ workflow.
Consequences of Crowding: Increased LOS, increased LWBS, increased ambulance diversion, increased medical malpractice claims (by a factor of 5 if the patient waits more than 30 minutes to be seen)
Fixing crowding requires an enormous effort on all departments in the hospital. However, fixing our crowding problem will result in better patient outcomes.
Walchuk Study Guide Pediatrics

*Bacterial Pathogens by age

*Physiologic vs Pathologic Jaundice
Strep pneumo is the most common bacterial cause of otitis media in children.
Strep throat is very uncommon in kids <3years of age.

*Potts Puffy Tumor
A single CT has a 1:2000 risk in young children for causing a fatal cancer sometime later in life. A single CT has a 1:5000 lifetime risk of causing a fatal cancer in older children.

*Neonatal acne is most common around week #3.

*Erythema toxicum Erythema toxicum neonatorum[1] (also known as erythema toxicum,,[1] urticaria neonatorum and toxic erythema of the newborn[1]) is a common rash in neonates.[2]:139[3] It appears in up to half of newborns carried to term, usually between day 2–5 after birth; it does not occur outside the neonatal period.
Erythema toxicum is characterized by blotchy red spots on the skin[4] with overlying white or yellow papules or pustules.[5] These lesions may be few or numerous. The eruption typically resolves within first two weeks of life, and frequently individual lesions will appear and disappear within minutes or hours. It is a benign condition thought to cause no discomfort to the baby. (Wikipedia)
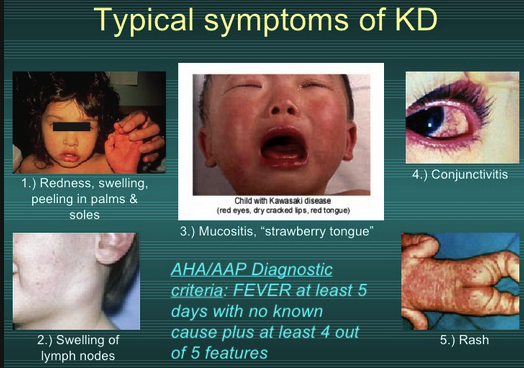
*Kawasaki’s Disease
0.3mg/kg po of decadron is equally effective as 0.6mg/kg of decadron for croup. So use the lower dose.
Alexander/Ohl/Einstein Discharge Pilot Project
We are trying to improve ED throughput. Optimize discharge process. Improve patient understanding and satisfaction.
Main interventions: Click Discharge Home but not Dr. Done. Print up DC instructions, work note, prescriptions. MD and RN go together to discharge patient. After discharge click Dr. Done in the computer.
There was good discussion about this proposed pilot plan. It will begin on Monday 1-11-2016