
Motzny EMS Study Guide

*Class A Bioterrorism Agents

*Alpha, beta, and gamma radiation

*Acute Radiation syndromes. Radiation=low lymphocyte count This is the earliest lab indicator of serious radiation illness.
Never approach a helicopter from the rear. There are dangerous rotating blades that can kill you. If a helicopter in on the slope of a hill, never approach or move away from the helicopter on the uphill side. Again the blades can kill you.

*START Triage algorithm. Triages patients on ability to ambulate, respiratory rate, perfusion (radial pulse) and mental status.
Anthrax is not transmitted person to person. Anthrax is transmitted by contact with the spore.
Ortho Cases

*Luxatio erecta. Highest incidence of neurovascular complications secondary to shoulder dislocations. Beware of axillary nerve palsy and axillary artery thrombosis.

*Ankle dislocation vs. Sub talar dislocation. Note that in the sub talar dislocation the talus remains in the mortise.

*Sub talar dislocation.

*Toddler fracture. Elise’s point is to follow the cortex of the tibia and look for a subtle incongruity of the cortex. Harwood comment: The only history you will get is the patient won’t ambulate. These injuries have no clinical clues on inspection of the patient’s extremity. There is typically no swelling or deformity to help you localize the injury. You just have to xray the length of the suspected lower extremity.
Splint with the knee in flexion to prevent rotation and prevent weight bearing.
Toddler's fractures or childhood accidental spiral tibial (CAST) fractures are bone fractures of the distal (lower) part of the shin bone (tibia) in toddlers (aged 9 months-3 years) and other young children (less than 8 years).[1] The fracture is found in the distal two thirds of the tibia in 95% of cases,[1] is undisplaced and has a spiral pattern. It occurs after low-energy trauma, sometimes with a rotational
component. (Wikipedia)
No need to call DCFS for toddler’s fracture.

*Bipartite patella is found most commonly in males and is located in the superior/lateral aspect of the patella.
OrthopedicWorkshop
Conference Notes 11-16-2016
Girzadas Intubating the Obese Patient
RapidOxygen Desaturation is our #1 Enemy This due to a decreased functional residual capacity and increased metabolic demand.

*Functional Residual Capacity is decreased in the Obese patient

*The Safe Apnea Period is decreased in obese patients due to rapid desaturation
Airway visualization is our 2nd Greatest Enemy
Aspiration is our 3rd enemy
• Decision #1 Head up positioning with RAMP or Reverse Trandelenburg optimizes FRC, VQ matching, and oxygenation. It also optimizes airway visualization and decreases risk of aspiration.
• Decision #2 Pre-Ox with BIPAP & Hi-flow Nasal Cannula
• Decision #3 Ketamine sedation/Topical, Avoid RSI and NeuroMuscular blockade. Maximize topicalization and minimize sedation. Larger/faster doses of ketamine can cause apnea in the critically ill obsese patient. So use doses like 20-50mg of ketamine given slowly and titrate to needed sedation level.
• Decision #4 Video laryngoscopy gives best first attempt success
• Rescue Device is Intubating LMA. Have it ready before you start.
• No Delay Cric. Be prepared to perform a cric before you sedate. If the patient is deteriorating and you are in a can’t intubate/can’t ventilate situation, Place the LMA and ventilate using that and commit to the cric and move quickly to get the cric done. You have only about a minute after the o2 sat gets to 90%.
• Decision #5 Ventilate 6 ml/kg (100kg) start with a PEEP of 5 and titrate as needed. Dave Barounis comment: no one needs more than 500ml tidal volume.
Patel/Tekwani/Williamson Vascular emergencies in the Pregnant Patient
Pre-Eclampsia
Pre-eclampsia can occur up to 6 weeks after delivery.
Mike Kennedy comment: Protein/Creatinine ratio has to be done using a straight cath urine.
Treatment is prompt delivery, control blood pressure, and supportive care.
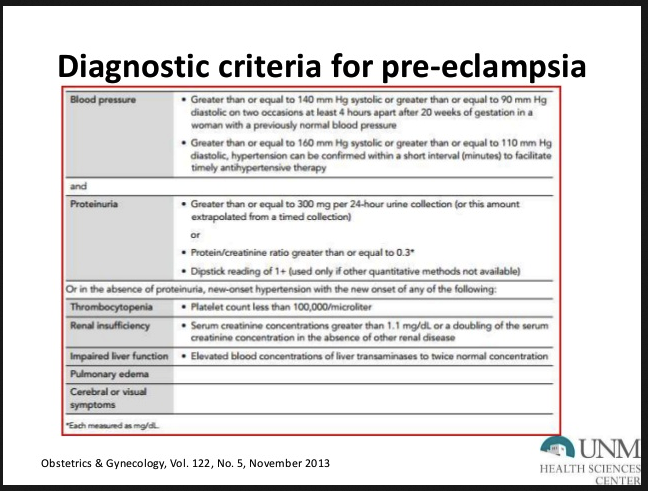
*Diagnostic Criteria for pre-ecclampsia
Asmita made the point that proteinuria and protein/creatinine ratio are specific for pre-ecclampsia but not sensitive. That means a lack of proteinuria or normal P/C ratio does not rule out pre-ecclampsia.
Any patient between 20 weeks of gestation out to 6 weeks post partum with a blood pressure >140/90 is pre-ecclampsia until proven otherwise. Check labs and consult with OB. At a minimum these patients need close follow up and an anti-hypertensive.
Aortic Dissection
Aortic Dissection can be due to hormonal and hemodynamic changes of pregnancy.
Diagnostic tests are CTA of chest, CTPE can also show signs of dissection, Trans-esophogeal echo is another test you can do to identify dissection.
If you are concerned about both dissection and PE, order the CTPE. If you write in the order notes you are concerned about both diagnoses the tech can do a double bolus study. The double contrast bolus can visualize both the aorta and pulmonary vascular tree.
Peripartum Cardiomyopathy
Peripartum Cardiomyopathy can occur in the last month of pregnancy out to 5 months after delivery. The clinical picture looks like CHF. Echo will show cardiomegaly.
Treatment is similar to CHF but you additionally have to anticoagulate due to risk of PE. Mortality is around 10% at 5 years. Only 50% recover at 6 months.
AMI can occur from plaque rupture, but can also be due to coronary artery dissection.
PE is more common post partum then antepartum.
Cirone STI’s
14% of all ED patients have at least 1 STI.
Nationally reported STI’s are gonorrhea, chlamydia, and syphilis. All these infections are on the increase. The Chicago area has seen a 2-3X increase in both gonorrhea and chlamydia.
If you see a female patient with HPV you should refer to gyne for colposcopy and cryotherapy.

*SyphillisThink about this diagnosis whenever you see a rash on the palms.
HSV lesions develop 2 weeks after contact. Patients have systemic symptoms with first episode (fever, chills, headache, myalgia). You can order Herpes serology panel if patients want it done. Most faculty just treat based on clinical diagnosis and do not order Tzank smears or serology. However, if a patient is adamant about getting tested to be sure about the diagnosis, the serology panelis probably the best test.
LGV is due to 3 types of chlamydia. Treat with Doxycycline.

*Disseminated Ghonorrhea. Make the diagnosis clinically and treat. If you want to do a test, do a cervical culture. Cervical swabs have the highest sensitivity compared to blood culture, swabs of the lesions, or arthrocentesis.
Denk DKA in the ED

*Look for hypokalemia findings on EKG in adult patients. Hypokalemia is the most common fatal electrolyte abnormality in DKA.
The bottom line diagnostic tests for DKA in all its presentations is ketonuria and increased anion gap. These 2 finding will be present in patients with straightforward DKA, euglycemic DKA, and mixed acid base disorders that include DKA.
Don’t intubate DKA patients if at all possible. You can’tmatch their minute ventilation needs with a ventilator. And they can get severely acidotic without adequate minute ventilation. They also have a high risk of aspiration. If they need oxygenation support you can use High Flow Nasal Cannula.
Don’t bolus insulin. There is no benefit and it can cause catastrophic hypokalemia in a DKA patient that you don’t have labs back yet and their K+ was already low unbeknownst to you.
I missed the remainder of Conference