
8:00 am Pediatric Appendicitis Update: Drs. Raghavan and Slidell
Pathophysiology:
Luminal obstructionà Increased pressure with continued mucus/fluid secretion à growth of bacteria, recruitment of WBCs/purulent fluid à higher pressures à venous outflow obstruction leads to wall ischemia à bacterial invasion of the appendiceal wall and subsequent extravasation of bacteria à “perforation”
5X higher rate of perforated appendicitis if 48 hour time of symptoms c/w less than 24 hours of symptoms
Complex/Complicated appendicitis:
Phlegmon, abscess, perforation or gangrene. +/- appendicolith.
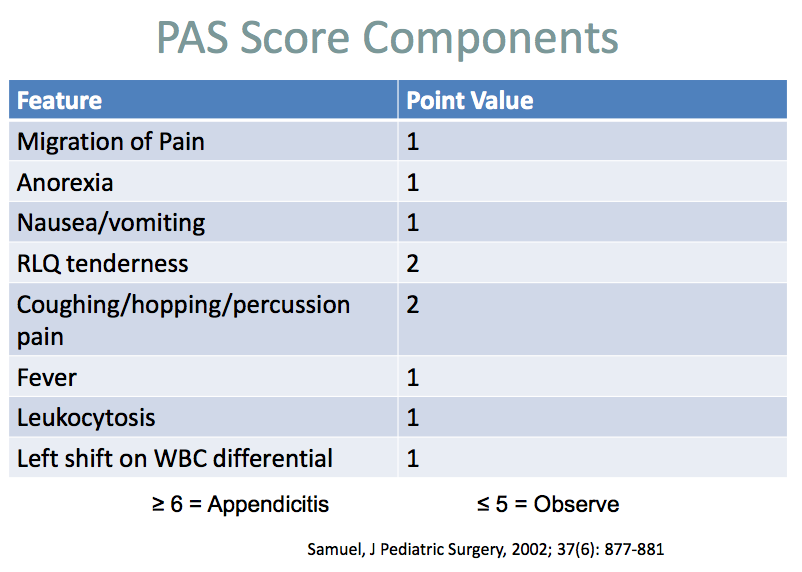
Pediatric Appendicitis Score (as opposed to Alvarado more used in adults)
8 components, total possible score of 10. Score does not include time; much less likely to be appendicitis if prolonged/intermittent pain.
Imaging Choices: US (fast/cheap/safe but operator and patient dependent), CT (accurate, makes other diagnoses, but radiation) MRI (accurate, but cost, time, availability). Each with pros/cons
Normal US: appendix less than 6 mm, compressible, no free fluid, normal hypoechoic muscular layer and echogenic mucosa, no peri-appendiceal inflammatory changes
Appendicitis on US: larger than 6 mm, non-compressible, hypervascular, appendicolith, associated findings of periappendiceal fat, free fluid, abscess, and point tenderness over appendix
Transverse and Lateral thickened noncompressible appendix on US= appendicitis


MRI gaining traction, accurate. Unlike in US, MRI can be called “negative” even if can’t see appendix, as long as no secondary signs of appendicitis on MRI
So far at ACMC: 100 cases in new protocol, with 30 positive cases by MRI, 29/30 true positives, 1 false negative
In general, more of a push for antibiotics/IV hydration, both while waiting for OR, as well as the potential for antibiotics as definitive care. Antibiotics are especially important in complicated appendicitis.
ACMC Pathway:
Start with Pediatric Appendicitis Score: PAS
PAS less/equal to 2 unlikely appendicitis
PAS greater/equal to 3 possible consider imaging (MRI if daytime weekday)
PAS >7 probable appendicitis, consider imaging, consult surgery and discuss antibiotics
As soon as diagnosis of uncomplicated appendicitis (no phlegmon, perf, abscess), then start Cefoxitin in the ED).
If complicated appendicitis then start Ceftriaxone and Flagyl
Basically, as soon as diagnosis of appendicitis is made, please start antibiotics, NPO, 1.5 x maintenance IVF
The future??? There will likely be another arrow in the pathway for uncomplicated appendicitis, with medical management using IV antibiotics only, as is reflected in evolving adult literature. Anticipated one-year success rate with IV antibiotics instead of surgery of 80%.
9:00 amM/M Dr. John Meyers
Case I: 17 yo female, MVC trauma patient 3 days prior seen at OSH, unremarkable initial eval, returned to ED with back/neck pain and vomiting. In ED with hypotension/tachycardia, developed fever, renal failure, ultimately with gram negative sepsis (EColi) due to UTI. Ultimately did well, renal function returned after treatment of sepsis. Received IVF, pressors, antibiotics, admission PICU.
Bias due to trauma history, one set of normal VS in ED (disregarded other multiple sets of abnormal VS). Patient given ketorolac (Toradol) in ED, which in retrospect not a good choice with the renal failure, hypotension. Was a good opportunity to switch from System I (intuitive) to System II (deliberate, reflective) thinking when initial evaluation and reaction the presenting symptoms don’t make sense. If stepped back, may have considered the differential of shock and reached diagnosis of sepsis more quickly.
Case II: Septic patient from NH.
Early central line placement, inadvertent arterial placement in femoral artery. Picked up by MICU nurse who read entire report of CT (mentioned “arterial line” in body of report). Teaching point-pay attention to your gut and any concerns about possible arterial placement. Confirm placement! Can use blood-column monometer (http://emcrit.org/central-lines/), or bubble test for IJ/subclavian (https://www.youtube.com/watch?v=XBNQw0BFJLI), or just US the wire to verify that wire is in the vein (both transverse and longitudinal views of the wire). Look at your imaging studies, and read the whole report!
Case III: Busy signout, in hurry to get to conference after overnight shift. Pending BMP on a patient that was signed out as “doctor done, nothing to do”, missed K of 7. Teaching point: signout is a dangerous time. Although signing out tasks for others to complete has negative juju, all outstanding labs and testing must be accounted for with a physician taking responsibility. Before hitting “doctor done”, look at all the data again. Remember, a new set of eyes can be very helpful-both for having coordinated signout of data, and to re-consider complicated/sick/undifferentiated patients.
10:00 am Fast Track Pitfalls-beware the snakes in the grass! Dr. Steve Anneken
Worry about these common/minor presenting complaints that are often missed on initial ED eval, that actually require urgent specialist followup, where outcomes may result in serious morbidiy for patient and medico legal exposure for the doc. Use dynamic stress testing with exam. Special xray views can improve sensitivity of diagnosis, CT when in doubt, and always look at your own images! If in doubt immobilize and refer, and carefully document your concern and plan of care/referral plan.
Top 12 MSK “snakes”
1. Game keeper’s or skier’s thumb-don’t worry about stress testing in ED, just splint and send to ortho!
2. Infectious Flexor Tenosynovitis-remember Kanavel’s cardinal signs. IV abx, early OR. Evil dorsal cousin....Human fight bite.
3. Recurrent branch of Median nerve “million dollar nerve” laceration. Think about it with laceration to palm at the base of the thumb/thenar eminence. Need to test opponens (opposition) strength. If concern, contact Hand. Needs repair within 2 weeks.
4. Snuff box tenderness, FOOSH, negative Xray = occult scaphoid fracture. Try axial load scaphoid pressure, and get scaphoid view xray, splint and send to ortho if unsure. Scapholunate dissociation another “miss” in that area. Use the “clenched fist view” xray to diagnose.
5. Elbow effusion (large anterior/”sail sign” or any posterior fat pad) without fracture on xray = occult fracture. 75% of fracture, long arm splint and ortho followup. Kids typically have occult supracondylar fx, adults usually have occult radial head fx.
6. Shoulder injury with lateral impact mechanism: posterior sternoclavicular dislocation. Rare, but can be clinically subtle, usually need CT to make diagnosis and look for associated injuries. Huge risk for mediastinal injury. Needs OR for reduction.
7. Quadriceps tendon rupture-sudden violent contraction of quadriceps with a slightly flexed knee-doesn’t require much force. Many not have a lot of pain if complete and may not have obvious deformity (swelling fills in the defect). Can’t lift heel off the cart! (extensor mechanism injury; other 2 possibilties are patella fracture and patellar tendon rupture). Xray with patella baja (low riding) in quads tendon rupture. Knee immobilizer, urgent ortho referral for OR, best result if OR in 72 hours. Could also use US to help with diagnosis. Tibial plateau fracture also a potential low impact fracture, esp. in elderly and the obese. Obese also with higher rate of occult knee dislocation! Patella fracture most common knee fracture, usually from fall onto flexed knee; consider sunrise and oblique xray or CT.
8. “Twisted ankle” with widened mortise/medial tenderness and tenderness over syndesmosis (squeeze tib and fib together about 6 inches proximal to ankle = squeeze test) concern for Maisonneuve fracture. Need to get tib/fib xray to look for associated proximal fibula fracture! Usually need operation.
9. “Twisted ankle” with lateral tenderness...think of peroneal tendon dislocation. More common in past with low ski boots. Other mechanism when walking down stairs, feels “snap.” Posteriorly located peroneal tendon ruptures, will have tendernessposterior to the posterior mallelous rather than anterior to malleolus as typical for simple sprain. Can do a physical exam stress test of the tendon.
10. “Snowboarder’s fracture”, when lands after jump, fracture of the lateral process of talus. Looks like a little chip, missed as an ankle sprain, tenderness is in the same spot as sprain. Look carefully at mortise view. May need OR.
11. Jones vs. Avulsion (Dancer’s) fracture of based of fifth metacarpal . Distinction if fracture goes into cuboid space (Avulsion) vs intointer-tarsal space (Jones). Danger of Jones = non-union, needs immobilization, non-weight bearing, and possible OR. Avulsion fracture can walk in a cast shoe. Also look for anterior process of calcaneus avulsion fracture.

12. Lisfrance: Can do weight bearing stress view xrays to help with diagnosis. 5% will also have compartment syndrome.
11:00 am Safety Lecture Dr. Nathan West: Morphine, Dilaudid, Fentanyl Oh My! Opioid safety.
--Remember different potencies of opioids, and mg vs mic dosing for morphine/dilaudid (hydromorphone) vs fentanyl.
--Morphine:Dilaudid 7:1 potency ratio. Assess your patients within minutes of medication dosing to determine effect/need for more meds.
--Duration of action 3 hours for morphine/dilaudid, one hour for fentanyl.
--Higher risk patients for adverse effects: extremely of age, obesity with risk of sleep apnea, opioid naïve, concomitant use of other sedation drugs, preexisting cardiopulmonary disease/major organ failure, thoracic trauma/incision/disease that may impair breathing.
--safety story of delayed apnea after ketamine and dilaudid administration
--Joint Commission recs: identify tolerance, find hidden fentanyl patches, opioid pumps, consider starting non-narcotic, goal of tolerable pain, if opioid naïve, start low and go slow. Take extra care when dosing patients who are being discharged. Avoid using opioids to meet an arbitrary pain rating.
11:30 am Dr. John Meyers Wilderness Medicine Elective/Avalanche Awareness course
Great stories, great pictures, thanks!

Noon: 5 slide FollowupMatt DeStefani
64 yo female, healthy, usually completely independent, now confused, found at home, generalized weakness. H/o one month of abdominal pain, h/o kidney stones.
Exam: unkempt, slow to respond, obese, dry mucous membranes, diffuse abdominal tenderness no guarding.
Workup: Hypercalcemia, normal TSH, CT abdomen/pelvis with gyn tumor, metastatic disease.
Hypercalcemia: 90% due to malignancy or hyperPTH.
ECG short QT, J waves, arrthymia
Treatment IVF, correct K, Mg, bisphosphonates, calcitonin, hemodialysis. NO loop diuretics-will worsen dehydration/electrolyte disturbances
Mnemonic:
· Stones (renal or biliary)
· Bones (bone pain)
· Groans (abdominal pain, nausea and vomiting, constipation)
· Thrones (polyuria) resulting in dehydration
· Psychiatric overtones (depression, anxiety, cognitive dysfunction, insomnia, coma)
Patient received 3 liters NS, 150 cc/hr, IV zoledronate, Calcium normalized by HD#3, poorly differentiated adenoCA, started chemotherapty, d/c HD #20