
Garrett-Hauser/Schmitz Oral Boards
Case 1. 32 yo female with shortness of breath and abdominal pain. P=135, BP=235/125. Patient has prior history of PE, HTN, and Cardiomyopathy.
CXR shows congestive changes and cardiomegaly. Troponin is elevated.
CT showed thoracic mass between the aorta and vena cava. Diagnosis was extra-adrenal, intra-thoracic pheochromocytoma.

Very Quick Literature search found one paper describing 34 cases of pheochromcytoma. The above picture lists the number of patients with pheochromocytoma at each of the sites. 7 patients had extra-adrenal locations of their pheochromcytoma with 2 being intra-thoracic near aorta. It looks like these tumors are going to be in the adrenals or by a major arterial structure.
There was an interesting discussion of how to manage the HTN and Tachycardia associated with pheochromcytoma in the ED. The consensus was to use NTG or Nicardipine for HTN initially, and after BP was improved cautiously beta-block with esmolol or lopressor. If a patient has CHF or Asthma/COPD you need to be very cautious about using a beta blocker. Some faculty felt esomolol may be safer due to the fact it can be d/c'd rapidly if you have any unwanted effects. It would be wise to consult Cardiology for assistance with these complicated patients. All cases of pheochromocytoma need surgical consultation for removal of the tumor.
Case 2. 92 yo male brought in from NH for unwitnessed fall. Patient has history of dementia. He is agitated and combative. Vitals are normal. Patient has pain and deformity of shoulder.

Image shows a superior shoulder dislocation. A superior shoulder dislocation is very uncommon.
After reduction with traction/counter traction, the shoulder pop's back up out of place. Superior shoulder dislocations usually severely damage the rotator cuff making any attempts at reduction unstable. Surgery also is commonly not successful. These patients usually develop a non-functional or severely limitedshoulder joint.
Case 3. 11yo child fell from bike and won't walk. Vitals are normal except HR=125. Child is in pain. Child has a porta-cath for prior treatment of leukemia. Patient has right hip pain with associated ecchymoses in right inguinal region. X-rays were negative. CT of the pelvis showed an iliac artery injury. Vascular surgery was consulted for repair of the artery. Iliac artery injuries can result from handlebar injury to the anterior pelvis/hip region.
PharmD Acute Angle Closure Glaucoma

Clinical appearance of acute angle closure glaucoma

Increased intra-occular pressure develops when aqueous humor can't drain thru the angle. Definitive management is laser iridotomy that drills a hole thru the iris to allow aqueous humor to drain.
mnemonic for causes of Acute Angle Closure Glaucoma: SAMS PA= Sulfa drugs, Anti's (anticholinergic/antihistamines/antiparkinson's drugs/antipsychotis/anticoagulants), MOAI's, Sympathomimetics, Parasympatholytics, Antiarrhythmics
ED Treatment: Timolol drops (fastest action), wait 3 minutes then give brimonidine (alpha-agonist), when IOP gets down to less than 40 you can give pilocarpine. If IOP is above 40, give mannitol and acetazolamide. Treat pain with narcotics. Treat nausea with ondansetron. Consult ophtho for iridotomy.
Burns FAST and E-Fast Exam

EFAST exam or Extended Fast exam adds bilat lung windows to the standard FAST exam (RUQ, SUb Xiphoid, LUQ, Supra-pubic views) to check for pneumo/hemothorax.

RUQ view. Fluid in Morrison's Pouch

LUQ FAST image showing fluid between kidney and spleen
When you are getting a subxiphoid view, ask the patient to bend their knees so that their feet are flat on the cart. This will relax the abdomimal muscles and give you a better chance at a decent view of the heart.

Lung Views with EFAST using M-Mode. Left side shows normal lung. Right side shows pneumothorax.
Lambert Gallbladder and Renal Ultrasound

Important landmarks to assure you are visualizing the gallbladder are the right portal vein and main lobar fissure. For extra points, getting the right kidney in the image also helps assure that you have visualized the gall bladder.

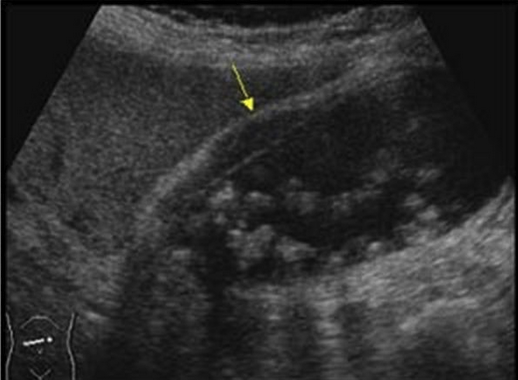
A Q&A between Elise and Mike brought out an important point. In the longitudinal view of the GB (G) you commonly will see the IVC (V) and just behind the IVC, the right Renal Artery (Arrow)
Acute cholecystitis with stones and wall thickening
Team Ultrasound Ultrasound Workshop
