
Lovell Procedural SedationJeopardy
Key Principles of Pain Management
1. Assess Severity 2. Use appropriate doses of analgesics 3. Titrate your pain meds 4. Monitor the patient's status.
Local anesthetics can be divided into amides and esters. Amides are longer acting. Amides have lower incidence of allergic reactions than esters. Amides all have two i's in the name (lidocaine, bupivicaine). Esters only have one i in the name (procaine). If a patient has an allergy to local anesthetics it is usually due to the preservative. Cardiac lidocane has no preservative so is usually considered safe in regard to allergies. Subcutaneous diphenhydramine can also be considered as a substitute for local anesthetic in the setting of severe local anesthetic allergy.
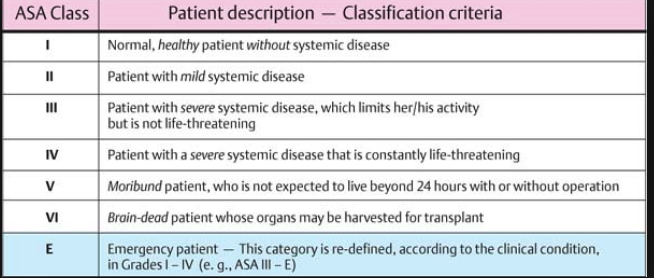
*ASA classification of patients for sedation and anesthesia
The risk of using ketamine in kids with an active uri is laryngospasm. If this develops you can bag the patient through this complication most of the time. Ketamine is OK in head injury. You can use ketamine in children down to 3 months of age for sedation. For patients younger than age 3 months ketamine is not approved and there may be a higher risk of laryngospasm.
3 drugs for treatment of regional complex pain syndrome: corticosteroids, calcitonin, and bisphosphonates. These patients present with burning pain, edema, warmth to skin, local sweating, and allodynia (pain to light touch). To treat, get the patient's affected limb re-mobilized (take off splint or cast) and start oral prednisone. They need follow up with PMR. If you don't identify and treat these patients early they can develop severe chronic pain.
Healthcare Disparity: A large study showed that African American pediatric patients had a 60% chance of getting pain medications for abdominal pain compared to white pediatric patients. In other words African American children were 40% less likely to get analgesia for abdominal pain compared to white patients.
Ways to reduce the pain of local anesthetics: 1. inject thru the open margins of the wound. 2. buffer with sodium bicarb 3. Inject slowly4. Warm the anesthetic5. Use a small (25 or 27 guage) needle 5. Reassure or distract the patient
Non-ASA NSAID's are noted by the FDA to cause heart attacks and CHF. Elise avoids giving NSAID's in elderly patients, patients with heart disease, HTN, or renal disease.
Benzocaine and prilocaine are the two local anesthetics that can cause methemoglobinemia.
Max dose of lidocaine is 4mg/kg without epinephrine or 7mg/kg with epinephrine. For bupivicaine, the max is 3mg/kg plain or 5 mg/kg with epinephrine. Girzadas comment: Draw up your local anesthetic before you enter the child's room so you never enter the room with a potentially toxic dose of anesthetic and the child does not see the needle.
Toxicity from local anesthetics initially causes dizziness, facial or extremity paresthesias, ringing in the ears. Patients may progress to seizures and then cardiovascular collapse (V-tach). Bupivicaine has the highest risk of cardiovascular toxicity. Treatment for local anesthetic toxicity is lipid emulsion therapy.

* Levels of procedural sedation

Recent large study in NEJM shows that if emergency physicians are high intensity opioid prescribers (prescribed opioids to 24% of their patients) the patients receiving opioids have a 30% higher relative risk of having long term dependence on opioids. Overall absolute risk of about 2% of becoming addicted. Elise comment: the pendulum has swung away from opioid use so be cautious of prescribing opioids to patients. Discuss with patients that there is a 2% risk of becoming addicted. Abhi comment: Warn patients about nausea and constipation to better inform them and encourage them to limit their use of narcotics.

Scoring system to determine who can be safely discharged after procedural sedation
KatiyarEM Billing and Coding
Optimizing your RVU's requires optimizing your documentation. Medical decison-making documentation is critical to your charting. Also make sure you write a procedure note for any procedures. Another key documentation item is to document your plan of care for a fracture or sprain. Also document a re-exam after a splint was placed to show neuro vascualar status is intact and the splint is not too tight. Ortho cases in general have high RVU's. Appropriate fracture and joint reductions have very high RVU values.
If you incise an abscess, probe, break down loculations and pack, that is considered a complex abscess.
Any wound checks following abscess drainage can be billed as a level 2 or 3. If you have to re-pack or give antibiotics, it becomes a level 3 chart.
Measure the length of the lacerations you repair. There is a ruler printed on the paper wrapping of a tongue blade that you can use to measure the wound.
If you make management changes with oxygen for a low pulse ox, document your thought process regarding the pulse ox and oxygen therapy. This is important for the medical decision making and for the RVU documentation.
The diagnosis you place on the chart is critical for determining the ED's case mix index. If you document acute STEMI rather than just Chest Pain it better characterizes the acuity your ED is seeing. Try to be as specific as you can in the ED. If the patient has an nSTEMI, document that diagnosis rather than Chest Pain. If the patient has DKA document that rather than hyperglycemia. If the patient has Pyelonephritis, document that instead of uti.
When you are describing patient behavior use objective terms as much as possible. For example, instead of writing the patient is "beligerent", write the patient was screaming obscenities at staff, violently rocking the cart and throwing punches at staff or other specific actions.
Review all chart documentation including what the nurses and the techs and EMS personel wrote. I any court case, the lawyers will go thru all charting with a fine tooth comb.
Marshalla Patient Safety LectureMassive Transfusion Protocol
We now have refrigerated blood in the ED for any patient in hemorrhagic shock. In that refrigerator there are 2 units of O pos blood for all males and for females over age 49. There are 2 units of O neg blood for females under age 49.
ED Attending physicians and Trauma Attending physicians can order blood from the ED blood supply for all causes of hemorrhagic shock. Only nurses can physically access the blood from the ED refrigerator.
Einstein ED EKG's
Noah discussed strategies to improve the information flow of EKG's in the ED.
Sedation Workshop
We broke into small groups and discussed different sedation scenarios.