
Thanks to Elise Hart for her help with the Conference Notes for the Ophthomology Lecture by Drs. Farooq and Shah this week.
Okubanjo/Ryan Oral Boards
Case 1. 19yo male passes out at a movie theater. No seizure activity identified. EKG shows a Brugada pattern.
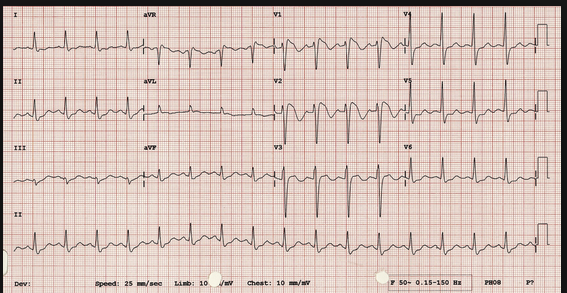
Brugada Pattern in Leads V1-2
Patient required admission to cardiolgy service for AICD placement.
Case 2. 41 yo male with right leg pain following a bad ankle injury. Vitals are normal. Xrays show maisoneuve fracture.
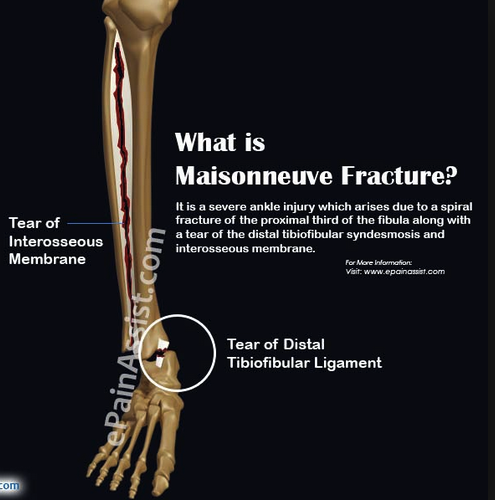
Maisoneuve fracture pattern has a medial maleolar fracture or tear of deltoid ligament with associated proximal fibular fracture and tear of the syndesmosis between the tibia and fibula. On exam, palpate both the ankle and the proximal fibula to identify this fracture pattern. Treatment is splinting followed by ORIF.
Case 3. 45 yo male with weakness and vomiting. Patient has tachycardia with thready pulses. Patient has history of daily ETOH use and recently has had vomiting and cannot keep down any food/fluids. Diagnosis is AKA.


Lovell Town Hall Meeting
Traylor Stroke Outcomes in Patients over 80yo Receiving TPA at ACMC
Logan gave his upcoming ICEP presentation. I did not want give away the info prior to his presentation. You will have to attend ICEP to get the outcome info.
Okubanjo Healthcare Disparities
Oyin gave her upcoming CORD presentation describing the Healthcare Disparities Curriculum she created.
Einstein Wilderness Medicine
Noah gave his upcoming CORD presentation describing the Wilderness Medicine Curriculum he developed.
Pastore 5 Slide F/U
There are 2 conditions in LVAD patients that require immediate notification of LVAD team.
#1 Pump failure which will be indicated by screaming LVAD alarms
#2 Pump thrombosis indicated by dark or brown urine. Patients will have an elevated LDH and signs of hemolysis on CBC. Patients may have new heart failure symptoms. The incidence of pump thrombosis has increased recently due to a trend toward lower anti-coagulation INR targets for LVAD patients.
Treatment of pump thrombosis is heparin drip and IV bicarb drip. Patient may go to OR for LVAD exchange or ECMO. TPA can also be used. Get the LVAD team involved in the patient's care as soon as possible.
Ashley recommended asking all LVAD patients what their urine looks like to screen for pump thrombosis/hemolysis. Also get an LDH on all LVAD patients to screen for pump thrombosis/hemolysis. Compare the LDH to prior levels.
Tran 5 Slide F/U
Treat delerium tremens with IV Ativan and IV phenobarbital.
Etoh withdrawal seizures don't typically have prolonged post-ictal periods.
The later a patient starts having withdrawal symptoms following cessation of ETOH, the worse the prognosis/severity of withdrawal.
Phenobarbital works at the GABA receptor and also lowers glutamate in the CNS.
Dexmedetomidine is a newer sedation medication that can be very effective in ETOH withdrawal. The downside is that it is very expensive.
Kennedy comment: When giving patients big time bnezo's and phenobarb keep them on an end-tidal CO2 monitor to be alert for potential apnea.
Hart/Regan Ortho Updates
Rotator Cuff Tears can be diagnosed with the following exams:
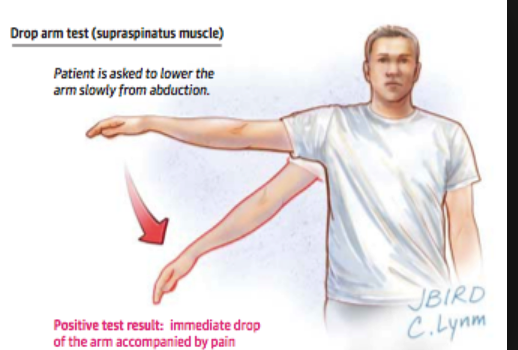

Treat with sling and Ortho Management. Some patients will require surgery
Farooq/Shah Visiting OphthalmologyConsultants from U of C Eye Emergencies
Ruptured globes - mechanism important. look for abnormality to pupil as one clue
Usually no rush to get FBs out unless contributuing to increased IOP (very rare) or if wood/vegetable matter (very inflammatory) - o/w FBs unlikely to get infected.
lateral canthotomy/cantholysis:
1) inject lido WITH epi to help w/ hemostasis/can also clamp down with hemostat
2) cut skin with 15 blade first (scissors often too dull, though )
3) Get scissor between globe and cathus, keeping dull side of scissor against globe. Cut posterior (lateral canthotomy) first (note this part doesn't do much for IOP), then inferior limb (cantholysis)
Pearls:
- If you can pry open lid and their EOMs are OK they're unlikely to need lateral canthotomy
- You can strum with scissors to see if you feel the cord of the tendon to know if you got it
- Don't worry too much about messing up the lid/skin - oculoplastics can always fix that later
- If pressure <22 they're probably fine
- On call Ophtho should come in if this is being done - OK to start without them, but their job is to ensure it was done adequately
- If being done for compressive optic neuropathy should also give steroids (recommended dose: 500 mg? solumedrol). Exception: Traumatic Optic neuropathy (posterior orbit sphenoid fx w/ effect on vision but not EOMs and not a lot of external swelling --> this involves direct trauma to optic nerve, akin to lack of efficacy of in spinal cord injury)
If there is a severe eyelid laceration exposing the globe, place antibiotic ophthalmic ointment as soon as possible to protect the globe. Talk to plastics or ophthomology to emergently approximate the lacerated lid to get coverage over the globe. If you as an emergency physician need to repair a gaping eyelid laceration that exposes the globe use 5.0 or 6.0 vicryl or 5.0 or 6.0 fast absorbing plain gut. Keep the sutures in the tarsal plane external to the mucosal lining as much as possible.
Injuries to the medial canthus area that damage the canaliculi system need to have a plan to repair the canulica within 3 days. Beyond 3 days there is significant scarring and it limits ophtho's ability to repair the problem.
Orbital floor fractures are almost never an emergency in adults unless there is an associated serious eye injury. Pediatric orbital floor fractures need to be addressed on an emergent basis because pediatric fractures under age 16 can entrap and strangulate the inferior rectus muscle causing life long diplopia. If a pediatric patient has inability to elevate the eye in the injured orbit they need emergent surgery.
Chemical Burns Check the ph in 4 quadrants of the eye. Check visual acuity, pupils, and eye pressure. Alkali burns cause more damage than acid burns because alkali causes liquifaction necrosis. Acute conjunctival irritation is actually a good sign, better than a whitish appearing cornea. Copious irrigation of the eye is the key management to chemical burns. Irrigate until the ph is 7 in all 4 quadrants. It may take 10-16L of NS to get ph down to 7. Chemical burns can cause severely elevated intraoccular pressure. Adjunctive therapy for chemical burns includes topical steroid, topical antibiotic, and cycloplegic drop. Other therapies include vitamin C, doxycycline, and intraoccular pressure lowering drops.
Central Retinal Artery Occlusion is characterized by painless unilateral vision loss. Patient should be admitted or stroke work up. Neurology should be consulted. There is no proven therapy for this disease. Occular massage may be helpful. Long term visual prognosis is poor. Rare diagnosis in children. Can be associated with malignacies or patent foramen ovale in children.
Globe rupture signs: 360 degree conjunctival hemorrhage, 8 ball hyphema, flat anterior chamber, irregular pupil. Get a CT scan to evaluate the globe. For adults, Avelox is the optimal antibiotic for globe rupture because of it's abilty to attain high levels in the globe. Levaquin is the second choice. In kids, discuss antibiotics with ophthalmology. Some pediatric specialists may advocate for a single dose of avelox in kids as well.
Acute Glaucoma treatment

Acute glaucoma management
Don't send topical ophthalmic anesthetics home with patients with eye pain. It can cause complete vision loss in the affected eye. For pain relief for corneal abrasions use topical antibiotic ointment and an oral analgesic.