
Cirone/Shroff Oral Boards
Case 1. 20 yo female presents with fever, tachycardia, and hypotension. Patient complains of right leg pain. Patient has necrotizing bullae on shin. Patient was at beach/ocean yesterday and had a skin abrasion on her shin that got infected.

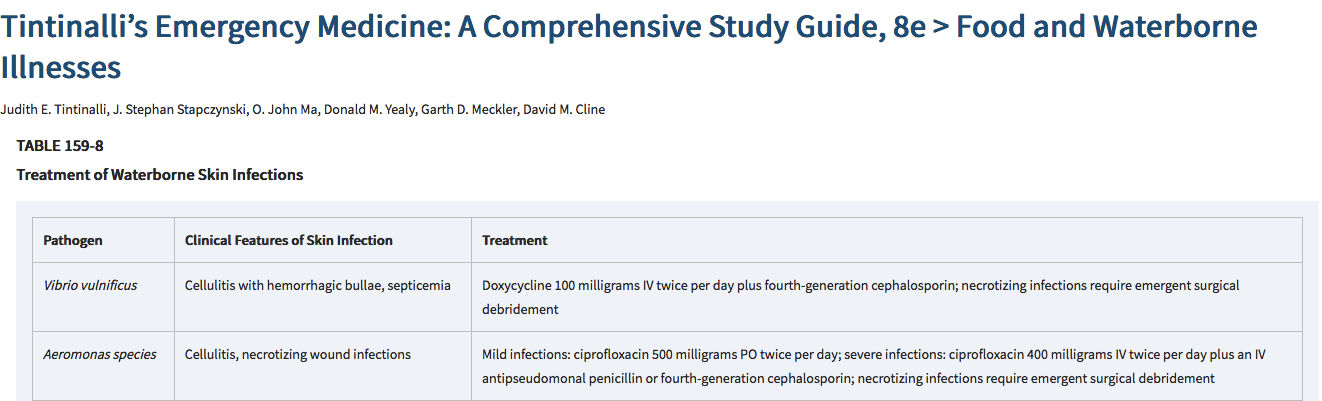
Vibrio cellulitis
Patient was treated for septic shock with IV fluids, IV antibiotics and norepinephrine.
Vibrio is gram negative bacteria seen in coastal waters. Vibrio can cause blistering cellulitis. Almost always occurs at site of prior wound. The infection can progress to necrotizing fasciitis. Tintinalli says: Treat with 4th generation cephalosporin combined with doxycycline. There is synergy with combining a 4th generation cephalosporin with doxycycline. If the patient develops necrotizing fasciitis they need emergent surgical debridement.
Dr. Lovell comment: For boards, bad infections associated with water are Vibrio for salt water and Aeromonas for fresh water. Make sure you treat with a 4th generation cephalosporin plus doxy or flouroquinalone.
Case 2. 25 yo male presents with altered mental status. Patient was bit by a snake the day prior in the everglades.

Red on yellow Kill a fellow (coral snake). Red on black venom lack.
Patient was treated with 3-5 vials of antivenin. If there is a definite coral snake bite, the patient should receive antivenin. If a patient has neuro symptoms, admit to ICU. Obtain a NIF to identify early respiratory weakness.
Case 3. 19yo male presents with foot pain due to injury playing basketball.

Jones fracture is also known as a Zone 2 fracture of the 5th metatarsal.
Jones fractures have poor blood supply and have risk of malunion. Treat with post mold, non-weight bearing, and orthopedic referral.
Treatment and Follow-Up
Patients with nondisplaced Jones fractures should be non–weight bearing in a cast for 6 to 8 weeks. Complications of a Jones fracture treated nonoperatively include bony nonunion, which may later require intramedullary screw fixation. Shock wave therapy has also been reported for treatment of nonunion.17 Some orthopedic surgeons are advocating for early surgical correction, especially in athletes, so posterior splinting and outpatient referral to an orthopedic surgeon are appropriate initial treatment.18 Nondisplaced avulsion fractures of the tuberosity, also known as a pseudo-Jones fracture, can be treated with a walking cast and pain control with weight bearing as tolerated. (Tintinalli 8th edition)
Burns Ultrasound Physics
Acoustic Impedance is due to the difference between tissue characteristics. If there is a large difference in impedance of two tissues the ultrasound image will be reflected or refracted and will limit the image. This is the problem with air and bone. Because air and bone impedance are so different from water, tissue, and blood, the ultrasound image is very negatively impacted by the air or bone.

Water, blood, and tissue all have similar impedances ranging from 1.48 to 1.7. Bone and air on the other hand have very different impedances from water, blood, and tissue. When bone or air is present in an ultrasound image, it will cause much reflection and refraction of sound waves degrading the image in the far field.

Gallstones are an example of a large difference of impedance between bile and stone. Distal to the bile/stone interface is only shadowing.
Gain adjusts the strength of returning echos (brightness). You want to have uniform brightness in both the near and far fields.
Higher frequency probes give better resolution. Lower frequency probes give you better tissue penetration. To image deeper structures, you may need to sacrifice some resolution to have deeper penetration of the sound waves.
Lambert Emergency Echocardiography
Mike's tip for imaging the subcostal view of the heart is to start in the right sucbcostal region and image the liver then rotate the probe to point at the left shoulder and you should be able to image the heart. Use the greatest depth to get this image. It's a long way from the RUQ to the top of the heart with this imaging window. So you need the greatest depth to see the heart from this window. Mike says the best subcostal images use the liver as a window to the heart. This is the best view to see pericardial fluid because you are looking at the base of the heart where dependant fluid would be.

Echo Windows: A. Parasternal long. B. Parasternal short. C. Apical. D. Subcostal.

Subcostal view of a large pericardial effusion

Large RV on Parasternal short axis view due to PE. Patient also has a "D sign" in which the large RV deforms the LV into a D shape.
Lambert Ultrasound in Trauma
FAST is basically a search for blood in the pericardium, thorax, or peritoneum.

E-FAST adds lung windows to the traditional FAST to look for pneumothorax.

RUQ view on FAST showing blood in Morrison's pouch and blood in the right chest cavity.

Looking for sliding of pleural line is critical to identify pneumothorax. With pneumothorax, the pleural line does not slide.
Lambert and Team Ultrasound Ultrasound Lab

