
Lorenz M&M
No Case Details, Just some take home points.
When you are wrong, admit it and move on.
“Any fool can try to defend his or her mistakes—and most fools do—but it raises one above the herd and gives one a feeling of nobility and exultation to admit one’s mistakes.”
― Dale Carnegie, How to Win Friends & Influence People
The secondary survey is critical in trauma to avoid missing more subtle injuries beyond that identified on the primary survey.
Paraphimosis: A retracted foreskin will block lymphatic drainage from the distal penis. As arterial inflow continues, lack of lymphatic drainage will cause a progressive edema of the penis distal to the retracted foreskin. As the foreskin continues to swell the phimotic ring becomes progressively tighter, and if not reduced, will eventually obstruct venous outflow. The distal penis will become painful and hyperemic. The edema will progress to ultimately obstruct arterial inflow resulting in penile ischemia, necrosis, and gangrene. This series of events, from retraction of the foreskin to arterial inflow obstruction, can occur over a few hours to 1 to 2 days. To relieve the obstruction, the phimotic ring must be advanced (reduced) over the glans of the penis. (Procedures in EM reference) This diagnosis can be confused with other GU complaints or overlooked. Be cautious not to miss this diagnosis.
Respect the risks of placing a central line. To verify placement of the line in the IJ, you can ultrasound the the IJ in the longitudinal plane. With the wire still within the vessel, angle the probe into the thorax and you can see the IJ widen into the right atrium. If you can visualize the wire in this area you know you are good. Alternatively, after pulling the wire, you can inject 10 ml of saline rapidly through the line and have an ultrasound probe on the heart to see turbulence in the right atrium and ventricle.

Kalnins NeuroRadiology
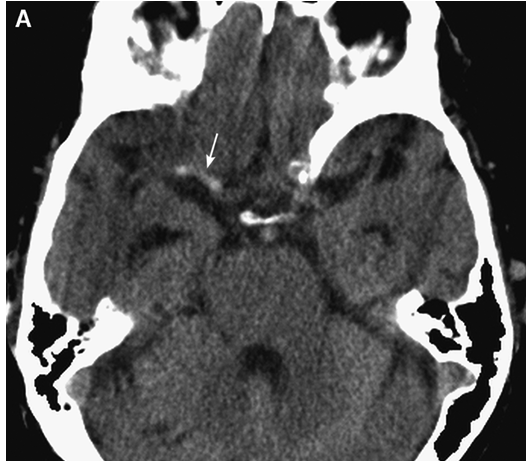
Dense MCA sign
A dense MCA sign corresponds to a significant acute clot in the proximal cerebral vasculature. Patients with this radiographic finding may benefit from neurointerventional procedures to aid in clot lysis or mechanical clot removal in order to reperfuse ischemic brain tissue. If you see this sign, consider consulting interventional neuro-radiology emergently.

Note the assymetry of the insular cortex from right to left. Dr. Kalnins emphasized the importance of the insular ribbon sign in identifying early stroke.
Dr. Kalnins recommended the website http://www.radiologyassistant.nl as a great resource to learn about radiology of all types. editors note: I googled it briefly and it looks outstanding.
Dr. Kalnins discussed cutting edge use of CT technology (perfusion, blood flow, cerebral blood volume, mean transit time studies) to identify early stroke.
Hawkins Interpreting CXR's
Unfortunately I missed this outstanding presentation.
Chiefs/EM Faculty Orthopedic Lab