Abnormal Echo
HPI: 75 year old man with past medical history of CAD s/p CABG, diabetes, hyperlipidemia and hypertension who presents to the ED from his cardiologist's office after an abnormal echocardiogram. He had no complaints of shortness of breath, chest pain, dizziness, lightheadedness, syncope; the stress echocardiogram was routine given his history of CAD.
Physical Exam: Clear S1 and S2 with no additional cardiac sounds including no murmurs, rubs, gallops. Lungs were clear to auscultation. The remainder of the exam was unremarkable.
Bedside Ultrasound:


-What is abnormal about this echo?
-How do you position the probe to obtain these echo views?
Our bedside ultrasound showed a well-circumscribed ovoid mass in the left atrium that moved with the mitral valve. Given the location and shape of the mass, it appeared to be a cardiac myxoma.
PARASTERNAL LONG AXIS
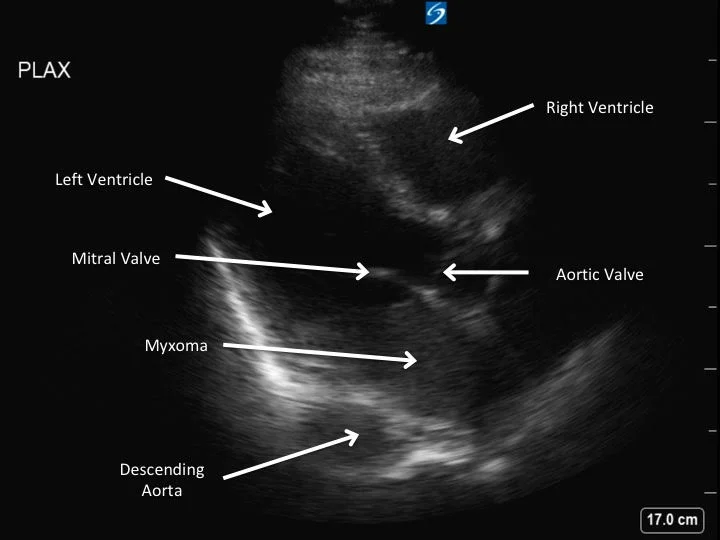
-Position the probe just lateral to the sternum in the left third or fourth intercostal space
-Troubleshooting tip: if visualization is difficult, consider placing the patient in the left lateral decubitus position to bring the heart closer to the chest wall.
APICAL 4-CHAMBER

-Position the probe at the cardiac apex approximately in the 5th intercostal space in the mid axillary line
-To avoid foreshortening the view, one should place the probe at the lowest intercostal space in the most lateral position to obtain a good view.
-Troubleshooting tip: if the patient is particularly skinny and the ribs are close together you can have them position their left arm above their head to expand the rib spaces.
Differentiating masses on echocardiogram: Masses noticed on echocardiograms are concerning for tumors (such as myxomas, papillary fibroelastoma, and carcinoid tumors), vegetations, and thrombi in the order of most to least common etiologies. One of the key differentiators is location. Thrombi are located in the left ventricle in patients with severe cardiomyopathy or ventricular wall aneurysms or mechanical valves. Migrating emboli would be noticed on the right side of the heart in the vast majority of cases. Vegetations need to be considered in the appropriate clinical situation, such as bioprosthetic valves or intravenous drug users and are most often on the upstream side of the mitral or tricuspid valves. Myxomas, the most common cardiac tumor, are predominantly in the left atrium. Given this key differentiator it is critical to get good views of all four chambers often using an apical 4-chamber view. Additionally, the parasternal long view can give a good view of the mitral valve (looking for vegetations), the left atrium (looking for myxomas), and the left ventricle (looking for thrombi). Lastly, using a parasternal short view one can visualize any of the valves as well as ventricular aneurysms and associated thrombi.
Noting the shape of the mass is also important. Vegetations and thrombi tend to be irregular in shape while the vast majority of myxomas have smooth surfaces and are ovoid or circular in nature. However, a small portion of thrombi can have smooth ovoid borders on ultrasound.
Cardiac myxomas: Cardiac myxomas account for nearly half of all cardiac tumors and are the most common benign tumor of the heart. Most are sporadic however there have been familial forms. They are more common in women with a 3:1 preponderance. They can be found in any chamber of the heart, but 75-90% occur in the left atrium. Often they are not found until they are 5-6 cm in size.
Cardiac myxomas can present with numerous symptoms. They can cause valvular obstruction leading to chest pain, pulmonary edema, shortness of breath with exertion and syncope. They can degenerate and cause embolic symptoms such as strokes in 30-40% of patients. Additionally, they can present with fevers, body aches, fatigue, weight loss and Raynaud's phenomenon. These constitutional symptoms are related to the myxoma's production of interleukin-6. In 20% of cases the individual is asymptomatic and it is an incidental finding.
Diagnosis is made via echocardiogram with transesophageal being slightly more sensitive and specific than transthoracic. CT and MRI are other diagnostic imaging options.
Urgent surgery is needed as patients are at risk of sudden cardiac death. Local recurrence happens in approximately 3% of cases and is higher in familial etiologies.
Conclusion: The patient was admitted to the hospital and had a transesophageal echocardiogram confirming a large mobile mass in the atrial cavity with appearance consistent with a myxoma. The patient went for myxoma resection on day 2 of his admission and discharged after 11 days in the hospital.
Additional resources:
-Au AM. "The cardiac mass: is it a thrombus, tumor or vegetation? Take it in the context of the disease" JBR Journal of Clinical Diagnosis and Research 2016; 4(1)
-Lone RA et al. "Atrial myxoma: trends of management." International Journal of Health Sciences 2008;2(2):141-151.
-Mendoza CE, Rosado MF, Benal L. "The role of interleukin-6 in cases of cardiac myxoma." Texas Heart Institute Journal 2001;28(1):3-7.
-Torregrossa J et al. "Ultrasound diagnosis of a left atrial myxoma in the emergency department." Western Journal of Emergency Medicine 2013;14(2):130-131.
-Kyle Bernard MD