
Airway Day
Much Thanks to Drs. Bolton and Tekwani and all the faculty for this outstanding Airway Workshop!!!
Mistry Approach to the Airway
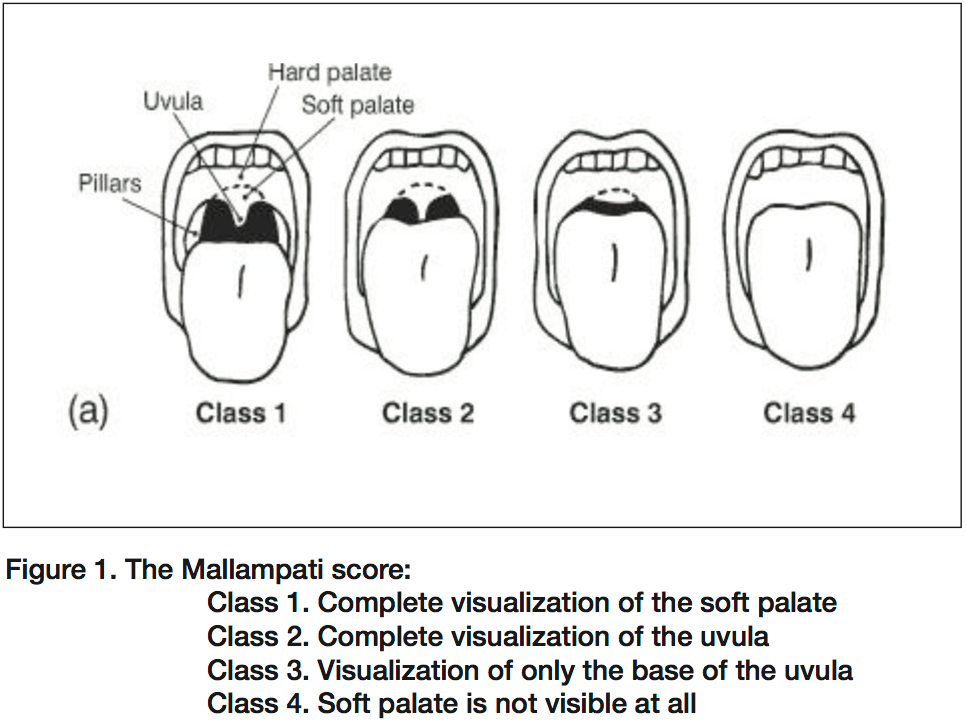
LEMON= Look, Evaluate, Mallampati, Obstruction, Neck Mobility. In the Evaluate section think 3-3-2: Can you fit three fingers in the mouth opening, three fingers from the chin to the hyoid, and two fingers from the notch of the thyroid cartilage to the hyoid bone? If you can’t do those three things that portends a difficult airway.
Your ability to keep calm during an airway emergency affects the demeanor and clinical capacity of the entire team
Build up an oxygen reservoir with 3 minutes of tidal volume breathing with high FIO2. Use a non-rebreather mask with the FIO2 as high as possible. 8 Vital capacity breaths will maximize airway/pulmonary O2 concentration and minimize CO2 concentration.
Bag Valve Mask Ventilation can be life-saving.
Laryngeal Manipulation: Intubating physician can move the larynx with right hand to optimize view and then have an assistant hold the larynx in that position. Alternatively the assistant can perform the BURP maneuver Backward/Upward/Rightward/Pressure.
Don’t forget to use the PEEP valve on the ambu-bag when bagging is difficult.
Nasal cannula in the nose with the oxygen flow as high as possible during intubation can increase the oxygen reservoir and buy you some extra time during intubation. The patient needs to be sedated during this technique as it is uncomfortable for the patient.
Don’t lay the severely dyspneic patient down until necessary. The sitting position can optimize their breathing.
Intubating the Obese Patient: Key is RAMP positioning. You need to elevate/position the external auditory meatus in line with sternal notch. You want the patient’s face looking up at the ceiling. You can use a combination of elevating the head of the cart and stacked linens to get the head positioned with the face looking up and the external auditory meatus parallel with the sternal notch.
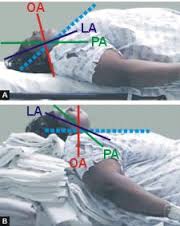
RAMP positioning
Sedated Laryngoscopy can be useful for the difficult airway. Ketamine sedation or Ketafol sedation in conjunction with good topical anesthesia of the throat and larynx is a useful approach if you have the time . Once you have the patient tubed you can then fully sedate and paralyze them.
There are many airway devices but, your knowledge and planning is the best tool you have to manage the difficult airway.
Lovell Airway Devices
Supraglottic devices such as an LMA can be an excellent bridge device for the difficult airway until you can get the patient intubated.
Elise dicussed numerous different airway devices.
In the patient who is unresponsive and won’t bite you, you can try digital intubation. You use your non dominant hand to feel the glottis and lift the epiglottis. With your dominant hand you pass the tube between your fingers and thru the cords.
Nasotracheal intubation: The patient has to be spontaneously breathing. You have to time the passage of the ET-tube to the patient’s inspiratory effort.
Gum Elastic Bougie should be your first “go-to” back up device. There are no contraindications to it’s use.
There was a discussion concerning the issue of whether video laryngoscopy will render direct laryngoscopy completely obsolete. Harwood and Elise felt that eventually it would make direct laryngoscopy obsolete although that is not the case currently. Old school Girzadas felt that direct laryngoscopy would always be a needed skill for the emergency physician.
Video laryngoscopy devices have been designed with increasing sophistication.
LMA is the bridge technique to temporize the airway until you can get the patient intubated. It is a blind technique that can be done in a few seconds in the crashing patient. It also can be the initial airway in the cardiac arrest patient. An intubating LMA can be used to get a definitive airway in the patient.
Cricothyrotomy is the procedure you have to be able to do as a last ditch technique. Biggest error is waiting too long. An assistant should be preparing for cricothyrotomy while you are still trying to intubate the patient. Can’t do cricothyrotomy on patients age 8 or below. Girzadas comment: You are usually performing this technique on obese patients. Due to adipose tissue and blood this is, in effect, a blind technique. You have to be able to feel with your fingers where you are going. Lovell and Girzadas comment: A bougie placed through the incision in the cricothyroid membrane will greatly help you keep control of the airway and place the shiley.
Elise discussed approaches to pictured specific difficult airways.
Sola comment: If there is a ton of blood in the airway and you can’t identify the cords, mild chest compressions can force some air through the airway and cause bubbling by the cords. Aim for the bubbles to tube the patient.
Advanced Airway Skills lab

