Conference Notes 7-9-2014
Lambert U/S Image Acquisition and Instrumentation
Medical use ultrasound is very similar to sonar used for naval/submarine applications. Sound waves are sent out of the transducer and the sound waves reflect off objects. The ultrasound machine measures the time it takes for the sound wave to return and creates an image based on these time differences as well as the number of reflections from objects of different densities.
On the ultrasound screen, the objects closest to the probe are located at the top of the screen (near field). More distant objects are lower on the screen (far field). The more echos that an object/organ reflects to the probe, the brighter the object will be on the screen.
Acoustic impedence depends on the density of the tissue and the speed of U/S in tissue. These differences account for varied images you see on the screen.
Ultrasound waves travel very slowly in air compared to soft tissue. This tends to scatter the sound waves and lessens image quality. That is why air in the bowel/lung are the enemies of the ultrasonographer
The curvilinear probe is the “work horse probe” for the emergency physician It is a low frequency probe that has a greater depth of ultrasound penetration into tissue but less resolution. This is good for imaging the abdomen.
High frequency linear probe has less depth of tissue penetration but higher resolution . This is good for identifying more superficial structures such as abscesses, vessels, and foreign bodies.
Low frequency sound waves have greater depth penetration but less resolution. High frequency sound waves have less depth penetration but greater resolution.
Near field: Top half of the screen image.
Far field: Bottom half of screen image. You loose some resolution in the far field due to loss of sound energy and more widely dispersed sound waves.
Phased array probe is different than other probes. It’s crystals are not arranged in a linear fashion like the curvilinear or high frequency linear probe. This probe has a very narrow field of view in the near field and a wide view in the far field. It is excellent for finding a window of view through ribs.
Conventional Ultrasound planes: The dot on the screen points to the head in the longitudinal/sagital orientation and to the patient’s right side in the transverse /axial orientation. The coronal plane is similar to longitudinal/sagital plane but the probe is on the side of the body.

*Imaging planes
Hyperechoic: An object causes more ultrasound reflections than the surrounding tissues. Hypoechoic: An object that causes less ultrasound reflections than surrounding tissues. Anechoic: an object causes no ultrasound reflections (example would be water).
High attenuating objects cause a lot of reflection of the ultrasound waves (bone, gallstones) and you get a shadow on the screen beyond this object. Ultrasound wave can’t get beyond this high attenuating object.

*Gallstone causing shadowing
The diaphragm can cause a mirror image artifact. You will see an image of the liver on both sides of the diaphragm. Same with the spleen when you image the left side.
Use the depth switch on the ultrasound machine to optimize your image on the screen. You want the object of interest to take up the vast majority of the screen.
Use gain buttons to optimize the brightness of your image. The ultrasound machine has controls for gain in the near field, far field and overall image.
You want to see your area/object of interest in two planes. You want to see the object to the extent of it’s boundaries.
Lambert FAST Exam
FAST=Focused Assessment of Sonography in Trauma. FAST is the best initial screening modality in trauma patient management
FAST exam has improved the decision making whether to take a trauma patient to the OR.
Indications: Chest or Abdominal trauma, Trauma in the Pregnant patient, Unexplained Hypotension.
The goal of the FAST is to find blood in the peritoneal cavity, chest cavity or pericardium. Can also look for pneumothorax in the chest.
Subcostal view is an effective way to look for pericardial fluid. Aim probe to patient’s left chin and probe indicator should be to patient’s right side. You are trying to obtain a 4 chamber view. Any fluid between the liver and heart in this view is in the pericardium.
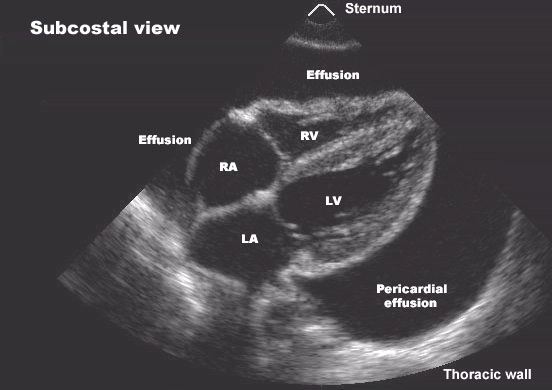
*Subcostal view with pericardial fluid
Next view is Parasternal long view of the heart. Try to get the image with apex of the heart to the left side of the screen. Fluid in the pericardium can be seen between the heart and the descending aorta.
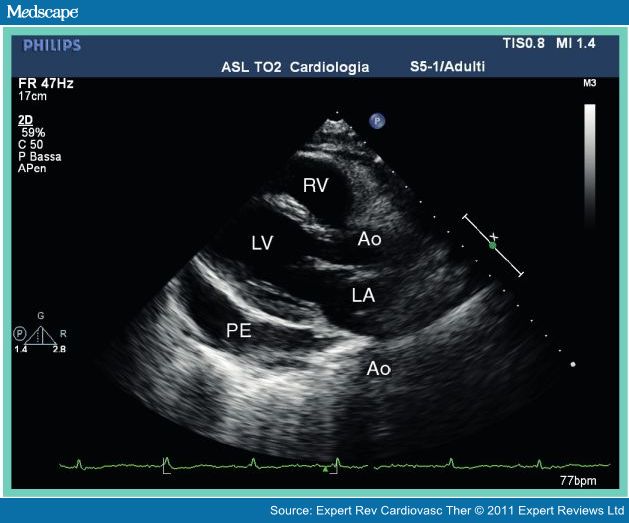
*Parasternal long view with pericardial fluid
Look for hemoperitoneum in Morrison’s pouch or the spleno-renal recess.

*Fluid in Morrison’s pouch between liver and kidney with the RUQ view

*Small Fluid in the spleno-renal recess
Last abdominal view in the FAST exam is the suprapubic window. Look for fluid posterior or around the bladder.

*Suprapubic view with fluid around bladder
Last thing to check is bilateral lungs for pneumothorax. Ultrasound is very sensitive and specific for pneumothorax (High 90’s% for both). Look for non-movement of pleura between the ribs.
FAST is primarily for the trauma patient but emergency physicians use aspects of the FAST for many other problems such as shock, ruptured ectopic pregnancy, and dyspnea.
Neal Lyons Update to Sepsis Order Set
There are new time expectations to get a lactate, give fluids, antibiotics (3 hours) and pressors and second lactate (6 hours)
Initial Fluid bolus is 30ml/kg
First line pressor is norepinephrine. Second line pressor is epinephrine. Elise comment: norepinepherine can be given peripherally at low dose until you get a central line placed. Low dose dopamine peripherally is no safer than norepinephrine peripherally.
Lambert and Team Ultrasound FAST Workshop
