Airway Day
Patel Airway Emergencies
Airway Assessment. You need to consider 4 things. Will it be difficult to BVM. Will it be difficult to Intubate. Will it be difficult to place a LMA. Will it be difficult to Cric?

Mnemonics to help answer the four questions above.
One thing not listed in all of these is pregnancy which makes all of these more difficult due to physiologic changes.

The LEMON method of airway assessment. Consider all these assessments when planning your approach to managing the airway.

3-3-2 rule

Mallampati Scoring
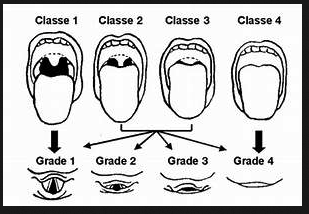
Mallampati is an imperfect marker of airway difficulty. A Mallampati 1 is predictive of a Grade 1 laryngeal view. Higher Mallampati scores are non-specific for which Laryngeal view you will get. If you have a Mallampati 4 you can expect a Grade 4 Laryngeal view (difficult).
If a patient has a neck hematoma or neck mass do not give a paralytic. If you do give a paralytic, the patient will loose any musle tone in their neck and will occlude their airway emergently. Instead use ketamine and topical anesthesia and then look with video laryngoscopy or nasal/oral fiberoptic device.

Apneic oxygenation. 15L O2 via nasal cannula or even better you can use high flow nasal cannula O2. It has been shown to prolong the safe apnea time, raise the lowest O2 sat, and increase first pass success in ED patients.
When you are pre-oxygenating a patient keep them sitting up. It improves functional residual capacity. Don't lay them down until after you give your induction medications.
DSI (Delayed Sequence Intubation) basically is using ketamine 1mg/kg to calm the patient patient who is in too much distress to adequately pre-oxygenate. Giving ketamine may relax them enough to effectively pre-oxygenate with BiPAP and also allow you to optimize them hemodynamically. When the patient is optimized with better oxygenation and BP, move forward to intubation either with or without paralytic based on expected difficulty.
Lovell Airway Devices
Unfortunately I missed this outstanding lecture.
Airway Lab in the New ACMC Sim Center
Thanks to Liz Regan for the pictures!