Brief notes this week as I missed some parts of conference.
Residency Town Hall Meeting
Holland M&M
To protect the confidentiality of the cases, I will only discuss the “Take Home” points.
Be alert to framing bias. There can be critically ill patients that are triaged to the hallway or general care area. This can also happen on the general wards of the hospital. You have to be alert to the possibility of critically ill patients in non-critical care areas of the hospital.
When intubating a very hemodynamically unstable patient consider Ketamine to avoid hypotension.
Christine comment: Ketamine does increase myocardial metabolic demand so that may be a downside of Ketamine to consider.
For the hemodynamically unstable patient, have push dose pressors ready to go prior to starting intubation. In fact give fluids and pressors prior to intubation.
Pre-oxygenate with bipap and continuous hi-flow nasal cannula O2.

*Scott Weingart/Elani SalakidouApproach to the hemodynamically unstable patient who needs intubation.
If patient has an acute change in status, escalate the level of care to address that change.
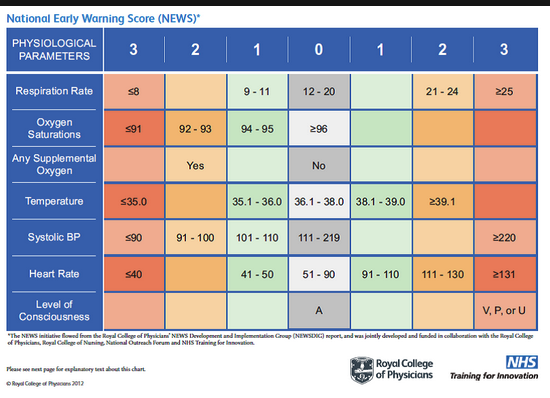
*NEWS Score (available on MD calc) can be used to determine who needs a higher level of care. Patients with a score over 7 have a higher potential to die or end up in the unit. This tool has a higher sensitivity than qSOFA in the septic patient. In addition it can be used in patients with disease processes other than sepsis.
Elise comment: If a patient has an O2 sat of 90% on a NRB that is hypoxia and you need to further evaluate the patient to determine the cause. Re-evaluation of the patient over time is critical to make sure the patient is stabilized.
Christine comment: Thinking back on cases that have bad outcomes should be constructive for the doctors involved, not destructive. We have to be careful how we think about our cases. We all want to be perfect but of course we are not. So we need to make sure our self-criticism is constructive and improves patient care and not self-destructive.
Garrett-Hauser Ethics
Case 14 yo female with abdominal pain and pregnancy. Parents are not aware patient is pregnant. Patient does not want you to discuss the fact that she is pregnant.
Illinois law allows teenagers to get care related to pregnancy without notifying parents. Shayla and Elise discussed ways to encourage the teenage patient to allow the doctor to fully disclose to parents. They advised telling the patient that it may be better to discuss this issue with your parents while you have the support and buffer of the ED staff. You can tell the patient that her parents will get her medical bills and will be able to see that she is getting pregnancy related care. You can make a call to the patient’s PMD and arrange follow up for the patient. This will give another opportunity for disclosure to the parents and also optimize the care of the patient.
Case. In cultures that revere extended families, you can ally yourself with other family members to accomplish therapeutic and communication goals. Shayla discussed a case in which the patient’s mom was so distraught that she could not function. Shayla allied herself with the patient’s aunt to accomplish communication and care goals.
ED Crisis Team Certificates
Holland/West ED Administrative Update